
Medication Data Challenges in TRACK-TBI: A Preliminary Analysis
We performed preliminary analysis on the medications from the patients in the TRACK-TBI consortia through a DUA established with the University of Cincinnati. For the subset of patients who underwent neuromonitoring in the study (n=124), there were 7,279 PRN medications requested at bedside and 4,772 scheduled medications. While PRN medications were represented as point administrations in the database, scheduled medications were represented as an interval with a start time, end time, and a free text administration frequency.
For one aspect of this project our goal was to time synchronize all of the medications for this cohort of patients with their corresponding neurophysiology. As you will see in this editorial, this task proved to be exceptionally challenging. Before performing any analysis, the scheduled medications had to be converted to medication administrations so they can be lumped with the PRN medications. Across all scheduled medications, there were 135 unique values for medication frequency. The 20 most common frequencies and 20 least common frequencies are shown in the table below:
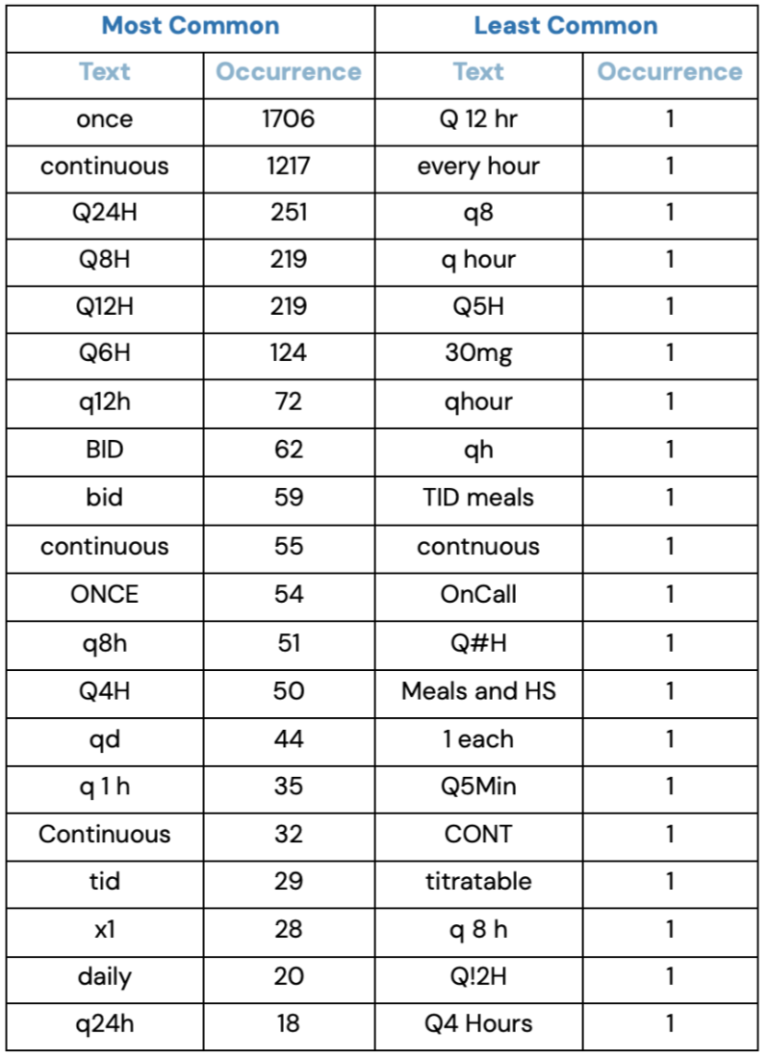
In a few cases, we noticed that the user mistyped the medication frequency such as with “Q#H”, which really means “Q3H” or “every three hours”–we think the user simply just held the shift key down for too long. In other cases, words were simply spelled wrong. See “contnuous” in table above.
Of the 138 medication frequencies, 44 could not be mapped to an absolute frequency. For instance, “qmeals” means “every meal,” but the absolute time point at which the medication with this frequency was administered is close to impossible to pinpoint. We can assume the times at which meals were given to the patient, but that wouldn’t be reliable. Examining other harmonization problems in the table above is left as an exercise for the reader.
These preliminary methods make a lot of assumptions that need to be verified. After these manually entered medication frequencies are comprehensively harmonized, a more comprehensive analysis can be conducted using the timestamps at which they were administered. Unfortunately, due to the data capture and data management system that was used during TRACK-TBI, harmonizing this data downstream has been incredibly difficult.



